
Laparoscopic Sleeve Gastrectomy
Laparoscopic Sleeve Gastrectomy
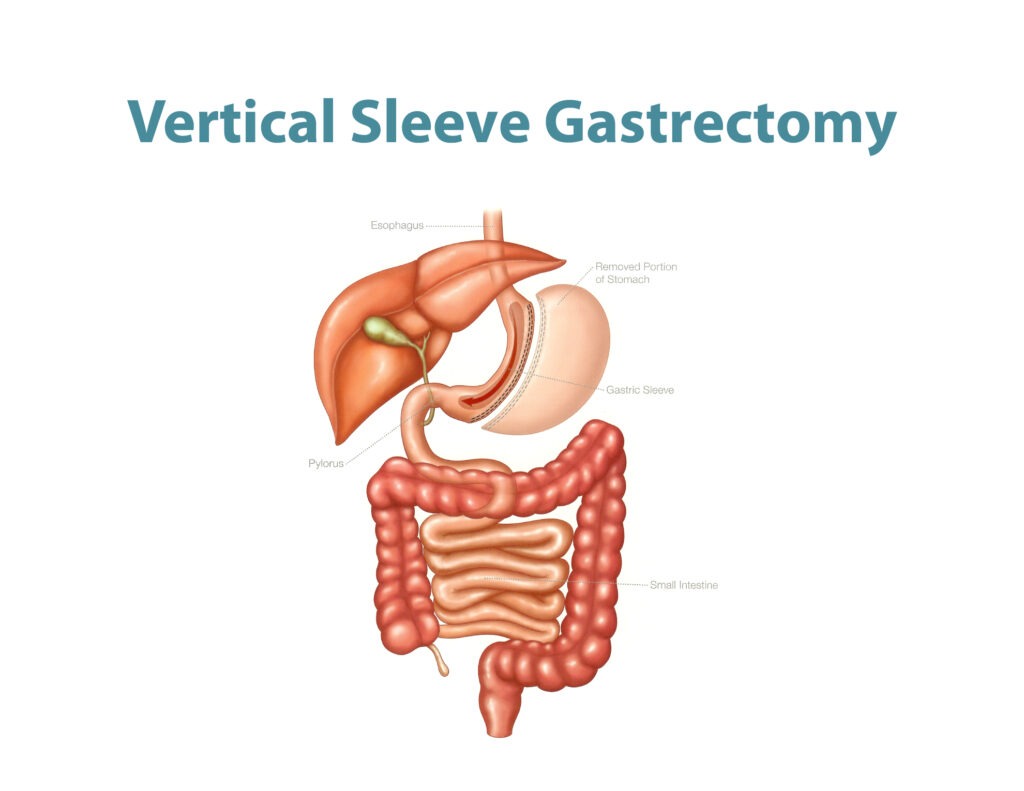
In this operation 75-80% of the stomach is removed, and the remaining will be a narrow stomach tube.
This is a relatively newer operation that has been done since the year 2004.
It was initially done as a first step to a second procedure for the patients with extremely severe obesity (BMI > 60 Kg/m2).
It proved its efficiency on its own, and since has been established as a solo procedure for the treatment of obesity.
Sleeve Gastrectomy has actually proved better results compared to the Adjustable Gastric Band, as weight loss is better (50-60%), and resolution of Type II Diabetes is also higher in 37-45% but does depend on weight loss.
This procedure does not include any bypass, so risk of malabsorption is non-existent.
It has no added risk of marginal ulcers or internal hernias as in the gastric bypass.
The main immediate complications are :
Leak: 1-2%, minimized by using 40 french bougie (sizer for cutting the stomach) which is done in our center.
If it occurs it requires additional operations for repair, possibly adding a stent from inside versus other drains.
If these measures do not control the leak, rarely it has to be converted to gastric bypass.
Bleeding: risk is similar to LRYGB.
Other late early complications :
Stenosis : narrowing of the stomach tube by 2-3%.
It is technically preventable by choosing the proper sizer and with proper technique.
If it occurs, it can increase the incidence of reflux and late leaks.
If short segment, it can respond to dilation through endoscopy, however if long segment it usually requires surgical cutting of the muscle layer only (myotomy) of the stenosis segment, and this usually can be done laparoscopically, versus converting it to Roux-en-Y gastric bypass.
As for late risks, they are :
Gastro-esophageal Reflux Disease (GERD) : in 25-30%, can be silent without symptoms, and newer international guidelines suggest the need for routine upper endoscopy after LSG to prevent and detect potential significant consequences of GERD.
Weight regain or inadequate weight loss : The rate of reaching > 50% of the excess weight loss (EWL) in this procedure is better than that of the band, and can be equal to the gastric bypass, in some patients, however, over the long run, some (25-30%) experience significant weight regain or not losing 50% EWL.
Vitamin and mineral deficiencies : all patients require long-term supplements and annual nutritional work up, as patients are at the same risk of deficiencies almost similar to gastric bypass patients.
Dr. Ayman Abdel Hameed :
The official page: Prof. Dr. Ayman Abdel Hameed, consultant and teacher of oncology surgeries and limited surgical intervention.
Doctorate in Oncology Surgery at the National Cancer Institute, Cairo University.
Master of Surgery oncology at the National Cancer Institute, Cairo University.
Bachelor of Medicine and Surgery, Faculty of Medicine, Kasr Al-Ainy, Cairo University, 2010, with distinction and honors.
More than 14 years of practical experience in surgery, oncology, and limited surgical intervention using surgical laparoscopes and surgical robots.
Book now : 01557112376