
Laparoscopic gastric mini bypass surgery
Mini gastric bypass surgery (laparoscopic)
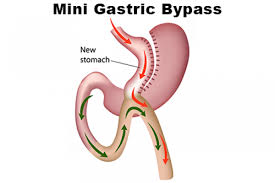
The mini gastric bypass, also known as the single anastomosis gastric bypass, is a relatively new procedure which combines some of the properties of a gastric sleeve and a Roux-en-Y gastric bypass.
The upper part of the stomach is divided into a tube, similar to the top three quarters of a sleeve and then joined to a loop of intestine.
It is an operation that combines restriction with some malabsorption and intended to result in good weight loss and improved quality of life.
What happens during laparoscopic mini/single anastomosis gastric bypass surgery ?
The mini gastric bypass, also known as the single anastomosis gastric bypass, is a relatively new procedure which combines some of the properties of a and a.
The upper part of the stomach is divided into a tube, similar to the top three quarters of a sleeve and then joined to a loop of intestine.
It is an operation that combines restriction with some malabsorption and intended to result in good weight loss and improved quality of life.
The mini-gastric bypass procedure is performed using laparoscopic (keyhole) technique under general anesthetic.
Five small incisions (between five and twelve mm in length) are made for the insertion of keyhole surgical instruments.
Using these instruments, the top of the stomach is stapled to form a thin tube (30ml to 50ml in size).
The thin tube becomes the new, smaller stomach and is completely separate from the rest of the stomach.
This stomach is then sewn to a loop of the small intestine, bypassing the first part of the intestine called the duodenum and approximately 150–200cm of the bowel.
The rest of the stomach and upper part of the small intestine remains in the body but is no longer used for food digestion.
Post surgery?
Most people will stay in hospital for three or four days after surgery.
After the procedure you will start on clear fluids only (water, black tea, broth, juices).
These will need to be sipped slowly in small amounts.
An x-ray study is performed after the operation to check the size of the stomach pouch and ensure there is no leak from the new connection.
You will then remain on fluids such as water, clear soups, milk, diet cordials, or tea and coffee for the rest of your hospital stay.
During the next four to six weeks, while your body heals, you will gradually increase the texture and volume of the food you take.
Further information, including a dietary guidelines booklet, will be provided at your post-operative appointment with the dietitian.
Does this surgery always lead to major weight loss?
The mini-gastric bypass procedure helps you to lose weight in two ways :
By dramatically reducing the amounts of food that can be eaten at any one time to a healthy portion size.
By decreasing the amount of calories you absorb from your food as a result of bypassing 150 to 200 cm of the upper part of the small intestine.
It is important to remember that surgery is a tool for weight loss. It is vital that eating behaviors are modified to get the best result from the procedure.
What are the possible complications?
As with any surgical procedure, the mini-gastric bypass operation has a risk profile which is important to understand before proceeding.
Bleeding – This occurs in less than 1 in 100 patients after the procedure.
This may require blood transfusion or rarely further surgery.
Infection – If an infection develops it may require treatment with antibiotics and can occasionally require reoperation.
Leaks at the staple line – This can at times require further surgery, occasionally in the first few days after surgery.
If these leaks persist they can become wounds (fistula) or be persistent infections within the abdominal cavity (abscesses).
If this complication occurs the length of stay in hospital can extend to weeks or potentially months after surgery.
This can be a life-threatening problem.
This occurs in less than 1% of cases.
Damage to organs – Any laparoscopic keyhole procedure can be complicated by unintentional injury to the organs near the area of operation.
This may require further surgery to repair the damaged organs.
Blood clots – Deep venous thrombosis (clots in the veins) and pulmonary embolism (clots in the lungs).
Pneumonia/ chest infection.
Your surgical team will take all possible measures to reduce these risks, but if these complications occur, further treatment may be necessary.